GLP-1 Decision Tree.
Whether to use a GLP-1, which one, how to dose, and how to come off without losing muscle on the way down.
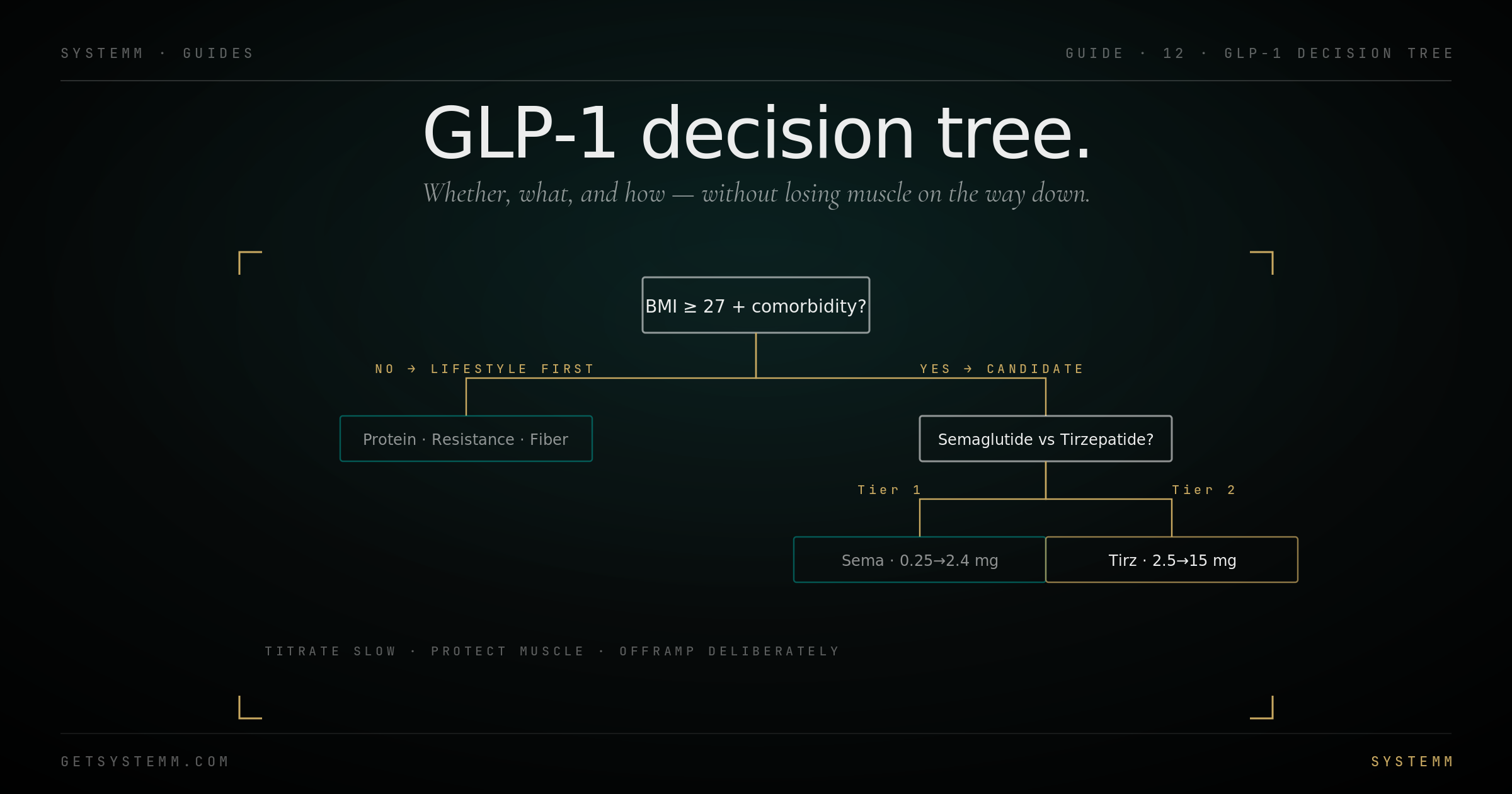
BMI, comorbidities, and the muscle question.
Clinical indications are clear. Off-label aesthetic use is where most users actually are.
FDA-approved indications: BMI ≥30, or BMI ≥27 with a weight-related comorbidity (hypertension, type 2 diabetes, hyperlipidemia, sleep apnea, fatty liver). Within these criteria, the risk-benefit is well established.
Off-label aesthetic use at lower BMIs (25–27) is increasingly common. The drugs work, but the risk-benefit shifts. Muscle loss as a fraction of total weight loss becomes a larger concern at lower starting body fat. Side effects don't scale down meaningfully.
Lifestyle first matters. If you haven't trained resistance 3x/week for 6+ months and you haven't dialed protein to 1g/lb lean mass, you're skipping rungs on the ladder. GLP-1s are extraordinarily effective; they're also extraordinarily good at masking poor lifestyle habits, until you stop, and the weight returns.
Semaglutide vs Tirzepatide vs Retatrutide.
Three drugs, three mechanisms, different magnitude and side-effect profiles.
Default choice for most people: Tirzepatide. Slightly better tolerated for nausea, larger absolute weight loss in head-to-head trials, but more expensive without insurance.
Semaglutide when cost or insurance constraints rule out Tirzepatide. Also when GI tolerance is a particular concern, some patients tolerate sema better.
Liraglutide rarely makes sense now. Daily injection, less weight loss, no real advantage.
Start low. Increase slow. Don't chase nausea.
The titration ladder is the FDA-mandated path for reasons. Skipping rungs causes the worst side effects.
Semaglutide titration: 0.25 mg weekly × 4 weeks → 0.5 mg × 4 → 1.0 mg × 4 → 1.7 mg × 4 → 2.4 mg maintenance. 16+ weeks to maintenance dose. Skip a step and nausea/vomiting becomes much more likely.
Tirzepatide titration: 2.5 mg weekly × 4 weeks → 5.0 mg × 4 → 7.5 mg × 4 → 10 mg × 4 → 12.5 mg × 4 → 15 mg maintenance. 24+ weeks to peak dose.
The minimum effective dose is the target, not the maximum tolerated dose. If you're losing weight steadily at 5 mg tirzepatide, there's no reason to push to 10 mg unless results stall.
- Protein: 1g per pound of lean mass per day. Non-negotiable on GLP-1.
- Resistance training: 3x/week minimum. Without it, 30–40% of weight lost is muscle.
- Hydration: 2.5L+ daily, GLP-1s suppress thirst alongside appetite.
- Don't push past 2 nausea levels, back off and stabilize.
The exit is harder than the entrance.
Stopping cold causes appetite rebound and weight regain. The taper protects what you built.
Don't stop suddenly after a long active phase. The body's adaptive response, increased ghrelin, decreased leptin, lower resting metabolic rate, is strongest in the weeks immediately following a major weight loss, and the GLP-1 is the thing keeping appetite in check.
Standard taper: maintain at peak dose for 3–6 months once goal hit. Then step down one rung every 4–8 weeks. Hold at each step until weight stable for 4 weeks.
During the taper, double down on lifestyle. Protein, training, sleep, food quality, these are the substrate that holds the result when the pharmacology comes off. Many users find some maintenance dose continues indefinitely; that's reasonable.
Plan for 10–20% rebound. The body fights back. Building 5–10 lbs of cushion above your target weight before tapering is realistic.
Related.
For educational purposes only. GLP-1 agonists are prescription medications requiring physician oversight. They carry warnings for thyroid C-cell tumors, pancreatitis, gallbladder disease, and severe gastrointestinal effects. Off-label use carries additional risk. Consult a qualified physician before initiating or modifying any GLP-1 protocol. This information does not substitute for personalized medical advice.