Longevity Lab Panel.
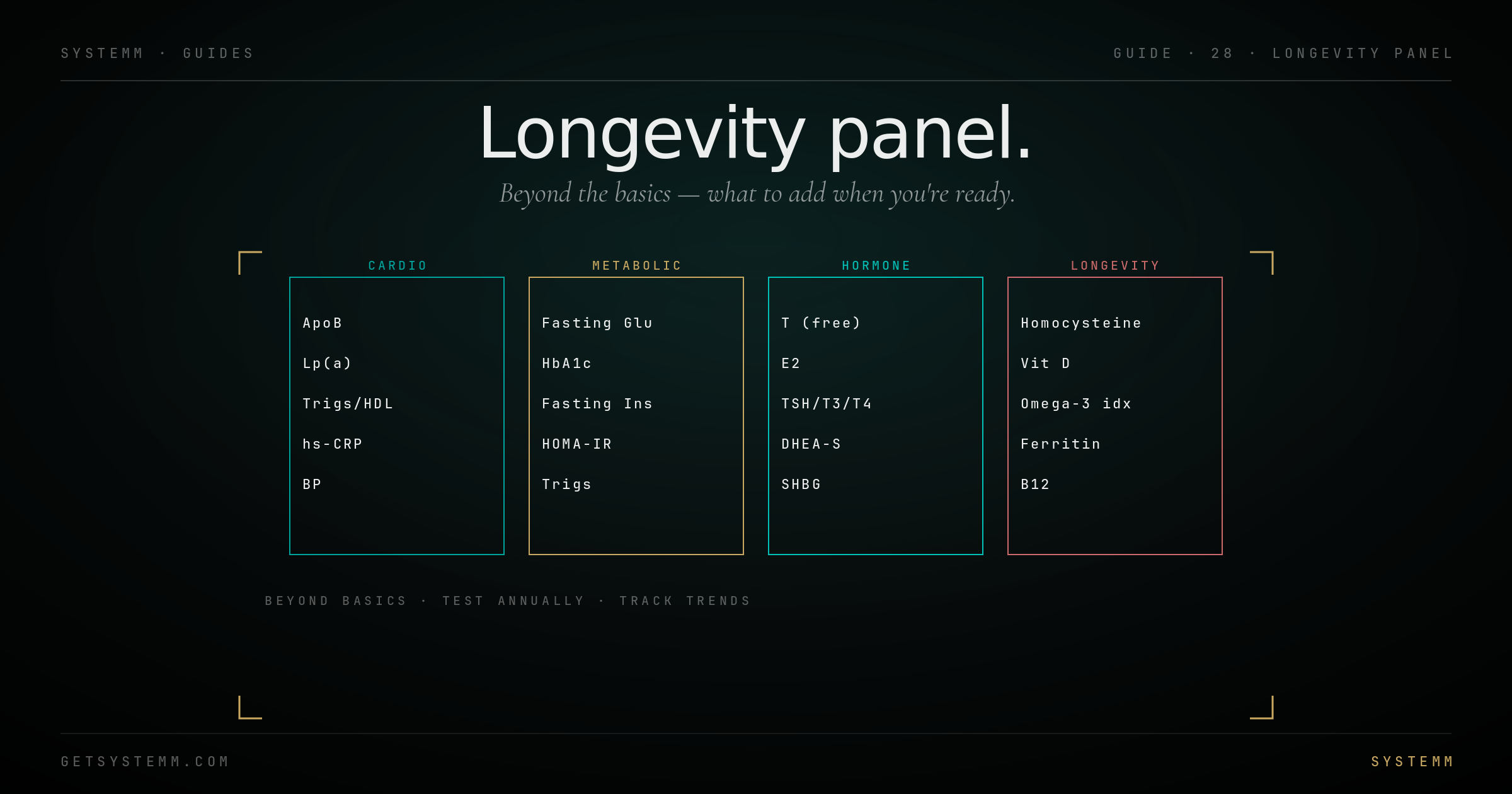
Beyond bloodwork basics. The 'go deeper' panel: ApoB, Lp(a), advanced lipoproteins, hs-CRP, homocysteine, omega-3 index. What each is, frequency, target values.
The basic panel misses the big risks.
Cardiovascular disease and metabolic dysfunction are detectable years before standard panels show problems. The longevity panel is the early warning.
Standard cholesterol panels (LDL-C, HDL-C, triglycerides) miss most of the modern risk picture. LDL-C measures cholesterol carried by LDL particles but not the particle count, and particle count is what predicts atherosclerosis.
ApoB measures the total atherogenic particle count directly. It's now considered superior to LDL-C as a cardiovascular risk marker by most lipidologists.
Lp(a) is a genetic risk factor that doesn't appear on standard panels. Elevated Lp(a) (>50 mg/dL) is independent of diet and exercise, it's largely genetic and changes the entire risk calculation. Test once in your life.
The longevity panel catches risks 10-15 years before they would show up on standard panels.
What to add.
Eight markers to add to your bloodwork-basics panel. Most are inexpensive and high-yield.
What moves which markers.
Specific levers for specific markers. Targeted interventions beat shotgun supplementation.
ApoB ↓: diet (reduce saturated fat, increase fiber), then statin or ezetimibe or PCSK9 inhibitor in sequence. The CV Risk Reduction protocol covers this.
hs-CRP ↓: lose visceral fat, address infections, address chronic stress, omega-3 supplementation, statin (CRP-lowering effect independent of LDL).
Homocysteine ↓: methylated B vitamins (methylfolate, methyl-B12, P5P-B6). MTHFR variants need methylated forms specifically.
Omega-3 Index ↑: fatty fish 2-3x/week or 2-4g EPA+DHA daily from supplement. Algae-based for vegans.
Fasting insulin ↓: resistance training, walks after meals, carbohydrate quality, sleep.
Uric acid ↓: reduce fructose and alcohol, increase vegetables, hydration. Allopurinol if persistent and symptomatic.
The most informative single test for CVD risk.
Once at 40, then every 5 years if >0. The score literally images plaque.
Coronary Artery Calcium (CAC) scan is a low-dose CT that measures calcified plaque in the coronary arteries. Score of 0 = essentially zero 10-year cardiovascular event risk regardless of other markers. Score 100+ = significant disease, even if labs look fine.
When to scan: men >40, women >50, or earlier if family history or elevated Lp(a). $100-400 out of pocket; most insurance won't cover.
What the score means: 0 = excellent; 1-100 = mild plaque, lifestyle focus; 100-400 = moderate, intervention warranted; >400 = severe, aggressive intervention.
The advantage: a score of 0 with elevated LDL-C is much less worrying than the labs alone suggest. Imaging trumps inference.
Related.
For educational purposes only. Lipid management, inflammation workup, and cardiovascular imaging require physician interpretation. Targets vary by individual risk profile and clinical context. This information does not substitute for personalized medical advice.