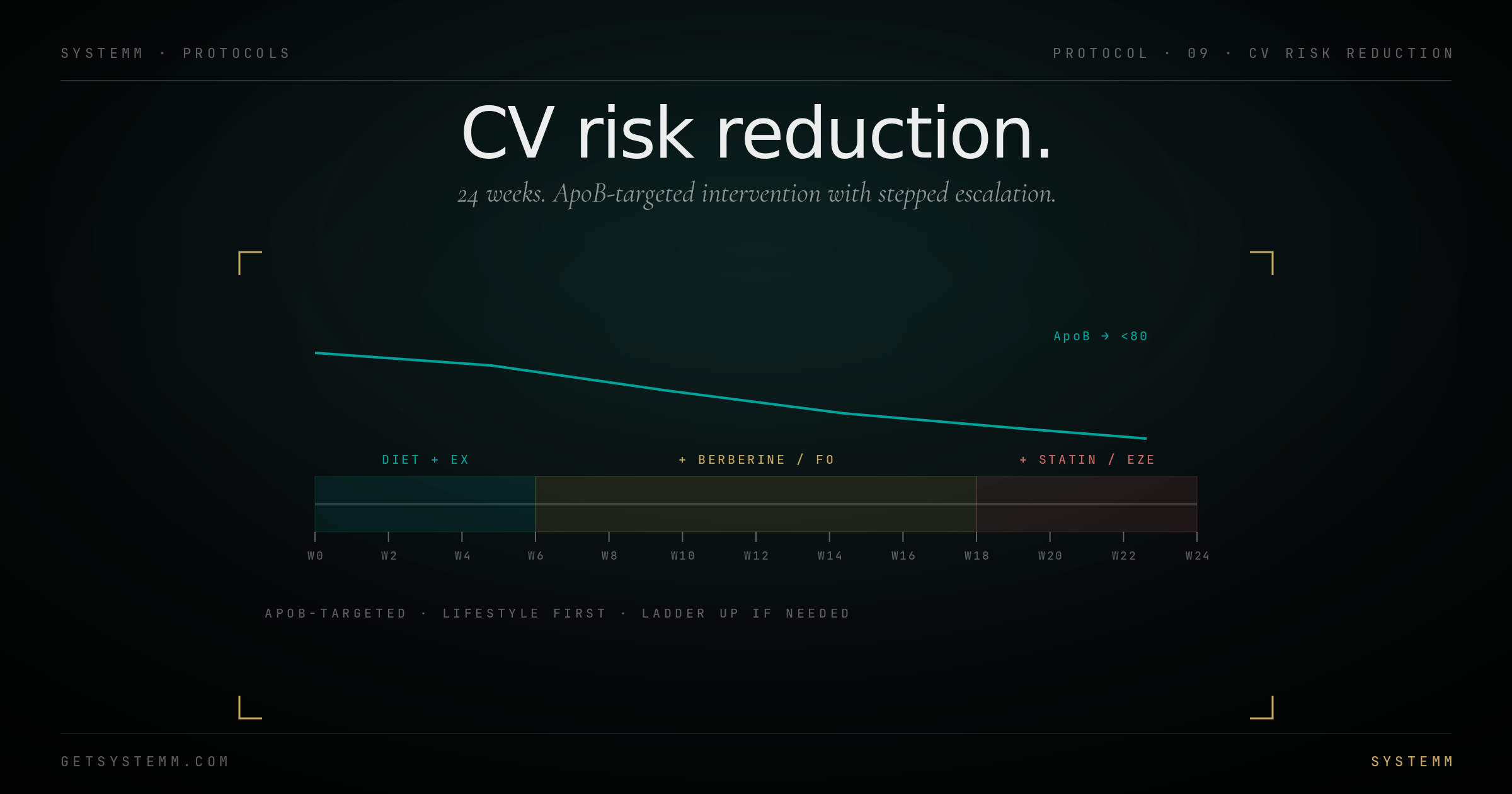
Cardiovascular disease is the largest killer in the developed world. It's also one of the most preventable when intervention starts early and is ApoB-targeted. This 24-week protocol takes ApoB from whatever you start with to below 80 mg/dL — the threshold below which atherosclerosis progression slows or halts.
01 · BASELINE
Get the data.
Standard lipid panel isn't enough.
- ApoB (the headline metric)
- Lp(a) — once, lifetime — genetic risk modifier
- Standard lipids (LDL-C, HDL-C, triglycerides)
- hs-CRP (inflammation)
- Homocysteine
- Coronary Artery Calcium scan ($100-400) — direct plaque visualization
02 · PHASE 1
Weeks 1-6. Diet + exercise base.
Lifestyle first. Many users hit target with this alone.
Diet: replace saturated fat with monounsaturated (olive oil) and polyunsaturated. Limit ultra-processed foods. Mediterranean pattern works.
Fiber 30-40g daily: soluble fiber (oats, psyllium, legumes) lowers ApoB by reducing cholesterol reabsorption.
Exercise: Zone 2 cardio 150+ min/week + resistance training 2-3x/week.
Retest at week 6: If ApoB is below 80 mg/dL: continue lifestyle, retest every 6 months. If above: phase 2.
03 · PHASE 2
Weeks 7-18. Add supplements.
Berberine, fish oil, plant sterols.
Berberine 1500mg/day (500mg 3x): modest LDL-C reduction, also lowers fasting glucose.
EPA+DHA 2-4g/day: lowers triglycerides 25-30%. Use a high-purity brand (Nordic Naturals, Carlson's).
Plant sterols 2g/day: lowers LDL-C 10-15%.
- Retest at week 12 and 18
- If ApoB below 80 at week 12: stay course
- If not declining by week 18: phase 3
04 · PHASE 3
Weeks 19-24. Medication ladder.
Statin → add ezetimibe → add bempedoic acid → PCSK9 inhibitor.
Statin (rosuvastatin, atorvastatin): most powerful single intervention. Side effects rare with rosuvastatin at modest doses (5-10mg).
Ezetimibe 10mg: blocks intestinal cholesterol absorption. Stacks with statin for additional 15-25% LDL reduction.
Bempedoic acid: oral, statin-alternative for statin-intolerant. Newer, more expensive.
PCSK9 inhibitors (evolocumab, alirocumab): injectable, expensive, reserved for genetic hyperlipidemia or statin failure.
- Discuss with physician (cardiologist or lipidologist if available)
- Targets: ApoB <80, or <60 if known atherosclerosis
05 · MAINTENANCE
After week 24.
- Recheck ApoB every 6 months once at target
- Continue medications indefinitely if needed
- CAC scan every 5 years
- Lifestyle base maintained regardless of medication
Disclaimer: Lipid medications carry side effects requiring physician monitoring. CAC scans involve radiation exposure (low dose, generally safe). Statins have important drug interactions. This protocol does not constitute medical advice — work with a cardiologist or lipid specialist.