If you've been on TRT and want to come off — for fertility, off-cycle, or to assess underlying production — this is the standard restart. Done well, most users restore endogenous T within 4-6 months. Done poorly, recovery takes years or never happens.
01 · BASELINE LABS
Before stopping TRT.
Get a comprehensive baseline. The starting point determines the protocol.
- Total + free testosterone
- LH, FSH (suppressed during TRT)
- Estradiol (sensitive assay)
- Prolactin, TSH
- Hematocrit, PSA
- Comprehensive metabolic panel
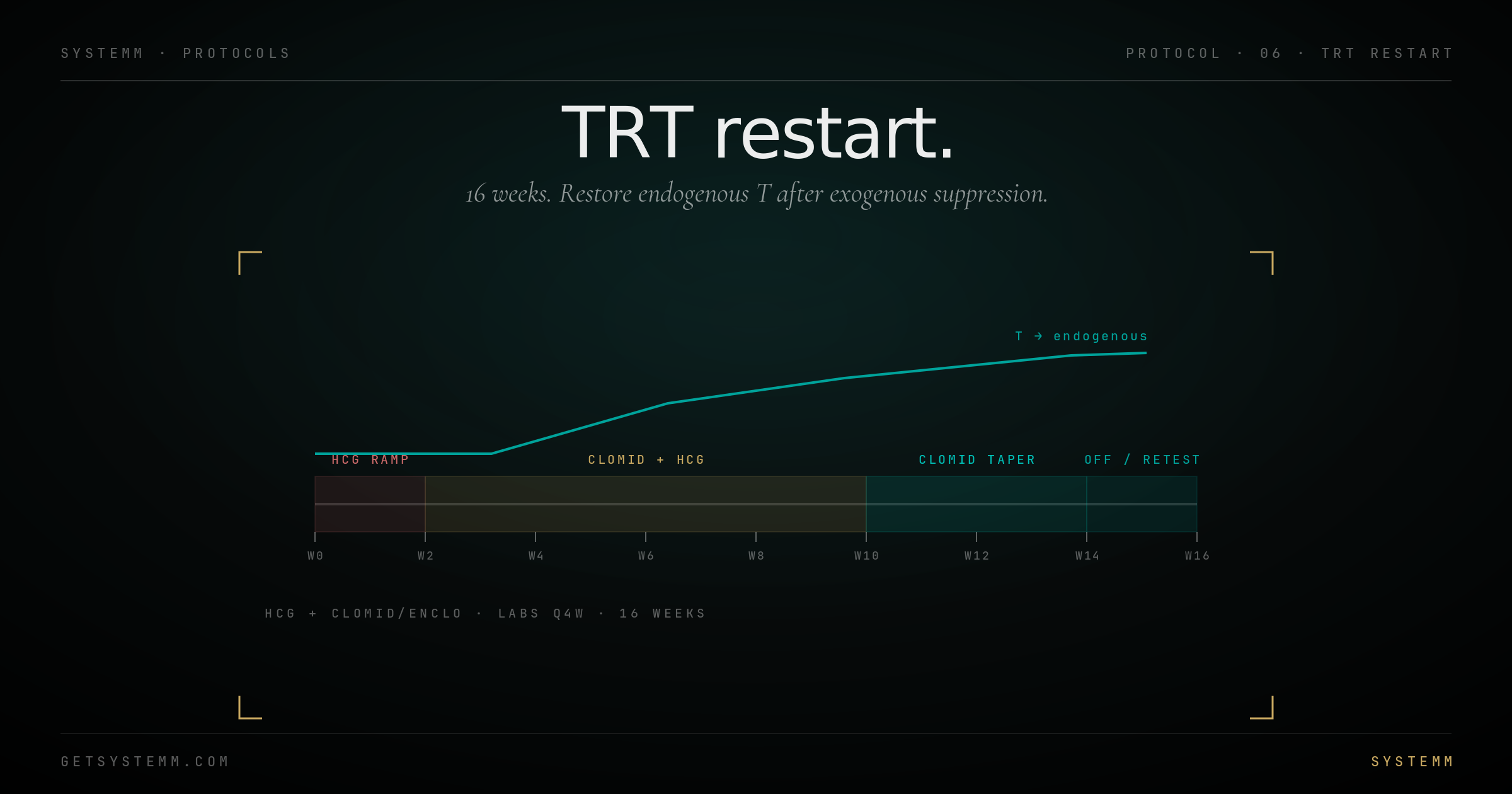
02 · PHASE 1
Weeks 1-2. HCG ramp.
Start HCG before stopping TRT. Maintains testicular function during transition.
HCG 500 IU subcutaneous, every other day. This stimulates testicular Leydig cells directly via LH receptors, preventing complete atrophy during the transition.
Continue TRT at standard dose during this phase. Stop testosterone only when phase 2 starts.
03 · PHASE 2
Weeks 3-10. Clomid + HCG.
Stop testosterone. Start clomid. Continue HCG.
Clomid (clomiphene citrate) 25-50 mg every other day. Blocks estrogen feedback at the hypothalamus, ramping endogenous LH/FSH.
HCG 500 IU 2x/week. Bridges the testicular function while pituitary recovery happens.
Enclomiphene as alternative to clomid — cleaner side-effect profile, same mechanism.
- Lab check at week 6: LH, FSH, T, E2
- Watch for clomid side effects: mood, vision changes, libido
- Adjust dose down if E2 climbs too high
04 · PHASE 3
Weeks 11-14. Clomid taper.
Drop HCG. Continue clomid alone at lower dose.
HCG off at week 11. Clomid 25 mg every other day, then every third day by week 13.
- Lab check at week 12
- Watch for testicular recovery via LH response
- Trust the labs over how you feel — symptoms lag chemistry by 4-8 weeks
05 · PHASE 4
Weeks 15-16+. Off and retest.
Stop all medication. Wait. Test.
Final labs at week 16, ideally also at week 20 and 24. Endogenous T should be 400+ ng/dL (recovery range) or higher.
If labs are low at week 16: re-evaluate. Some users need a second cycle. Some have primary hypogonadism that didn't recover — in which case TRT was the right answer all along.
Honest framing: Some men can restart endogenous T to normal levels. Some can't. The point of this protocol is to find out — not to guarantee an outcome.
Disclaimer: TRT restart involves prescription medications (HCG, clomid, enclomiphene) requiring physician oversight. Self-administration without medical guidance is dangerous and may permanently impair the HPG axis. This protocol does not constitute medical advice.