HPA Axis.
Hypothalamus, pituitary, adrenals. The stress-response loop. Cortisol comes from here, and so does the failure mode of chronic stress.
The body's emergency system.
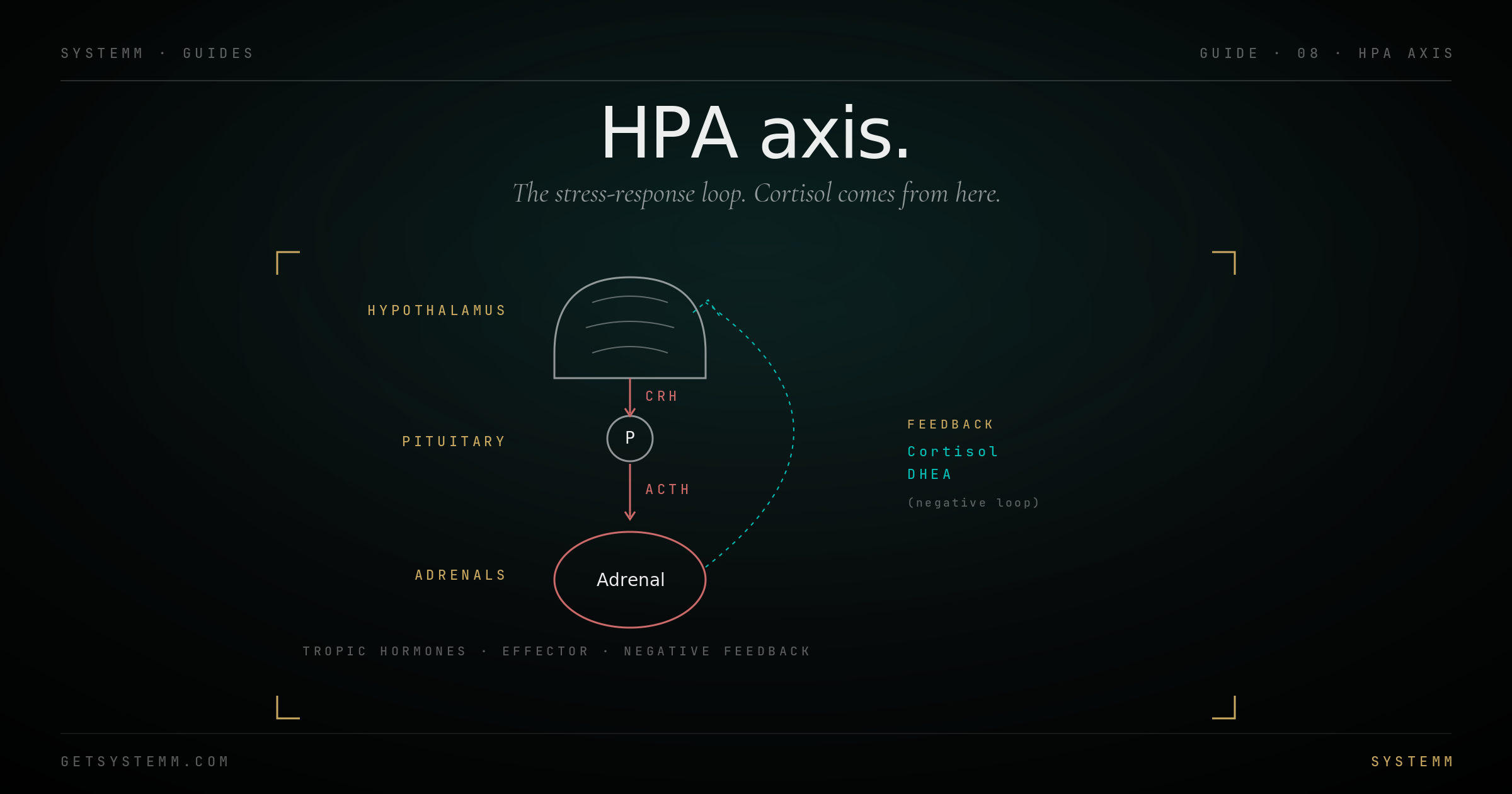
CRH → ACTH → cortisol. Designed for acute threats. Misused as a chronic input.
Stress hits the hypothalamus first. Real, imagined, physical, emotional, the brain doesn't distinguish. The hypothalamus releases CRH (corticotropin-releasing hormone) into the portal blood supply to the pituitary.
The pituitary responds with ACTH (adrenocorticotropic hormone), which travels via bloodstream to the adrenal cortex.
The adrenals release cortisol, your primary glucocorticoid. Cortisol mobilizes glucose, raises blood pressure, suppresses inflammation and immunity, and shuts down 'non-essential' systems (digestion, reproduction) so the body can deal with the threat.
Cortisol feeds back negatively to the hypothalamus and pituitary, normally shutting the response off as the threat passes. In chronic stress, this brake fails.
Two completely different problems.
Acute cortisol is a feature. Chronic elevation is the failure mode.
Acute cortisol (a tough workout, a deadline, a fight): rises within minutes, peaks within 60 minutes, returns to baseline within 90 minutes. This is normal and useful. The body literally cannot adapt to training without it.
Chronic cortisol elevation: persistent stressor or perceived threat that doesn't end. Cortisol stays elevated. Negative feedback dampens. Receptors downregulate. Then comes the cluster of downstream problems: belly fat, sleep disruption, suppressed immunity, blood sugar dysregulation, muscle loss, low libido, slow recovery.
HPA dysregulation isn't 'adrenal fatigue'. The popular term is misleading, the adrenals don't get tired. What happens is the brain (hypothalamus and pituitary) and the cortisol receptors adapt to chronic exposure. The system becomes dysregulated, not exhausted.
- Wired-but-tired feeling, anxious energy without endurance.
- Wake at 3–4am, can't get back to sleep.
- Belly fat that doesn't respond to diet/exercise.
- Catching every cold that passes through.
- Loss of morning erections in men (low T downstream).
- Cycle irregularities or amenorrhea in women.
How to actually measure it.
One serum cortisol tells you almost nothing. The pattern is what matters.
Salivary or urinary cortisol, four timepoints across the day. Morning (within 30 min of waking), midday, afternoon, evening. This shows the diurnal curve. Inverted = HPA dysregulation.
DUTCH test (dried urine total metabolites) is the most comprehensive, captures cortisol, cortisone, and major metabolites across the day, plus sex hormone metabolites. Best single test for HPA work-up.
DHEA-S is the adrenal androgen and a useful counterweight to cortisol. Chronic HPA strain often shows low DHEA-S relative to cortisol, the 'cortisol/DHEA ratio' is a common stress index.
What actually moves the needle.
Lifestyle base first. Supplements as nudges. Drugs only with a diagnosed pathology.
Sleep is the foundation. Seven-plus hours, consistent timing, dark/cool room. Without sleep, no other HPA intervention works. This isn't negotiable.
Stress modulation: breathwork (down-regulates sympathetic tone), meditation (10+ min daily, ideally morning), time outdoors (forest, sun, no screens). These aren't soft, they are direct vagal inputs that reset the HPA tone.
Training discipline: hard training is acute HPA stress. If chronic HPA strain is already present, dropping training intensity for 2–4 weeks is often necessary. Walking, mobility, light resistance only.
Supplements with reasonable data: phosphatidylserine (blunts evening cortisol), ashwagandha (modulates anxiety/cortisol), magnesium glycinate (sleep + stress). All adjuncts, not foundations.
Caffeine review: chronic high-dose caffeine in the context of HPA strain is jet fuel on a fire. Cut to morning-only or eliminate during a reset.
Related.
For educational purposes only. Chronic HPA dysregulation may signal underlying conditions requiring medical evaluation (Cushing's, Addison's, hypothyroidism, sleep apnea). Persistent symptoms warrant physician assessment. This information does not substitute for personalized medical advice.