Sun Protocols.
UV index, vitamin D timing, sunscreen choice, melanotan, skin cancer screening. The case for sun and the case against, both have merit.
Why morning sun isn't just a wellness meme.
UVB synthesizes vitamin D in the skin. Latitude, season, and skin color determine how much you get.
UVB triggers vitamin D synthesis by converting 7-dehydrocholesterol in skin to pre-vitamin D3. The reaction requires UVB specifically (not UVA), which is filtered out by glass, by latitudes above ~37°N in winter, and by SPF 30+ sunscreen.
10-20 minutes of midday summer sun on arms and legs produces ~10,000 IU of vitamin D in light-skinned individuals. Dark skin requires 3-5x longer for equivalent synthesis.
Practical implications: in temperate climates, store vitamin D from summer sun if you can. Supplement 2,000-5,000 IU D3 daily in winter or if you don't get direct sun.
Test 25-OH vitamin D once. Target 40-60 ng/mL. Below 30 = deficient. Above 80 = no additional benefit and some risk at very high levels.
When to get sun, when to cover.
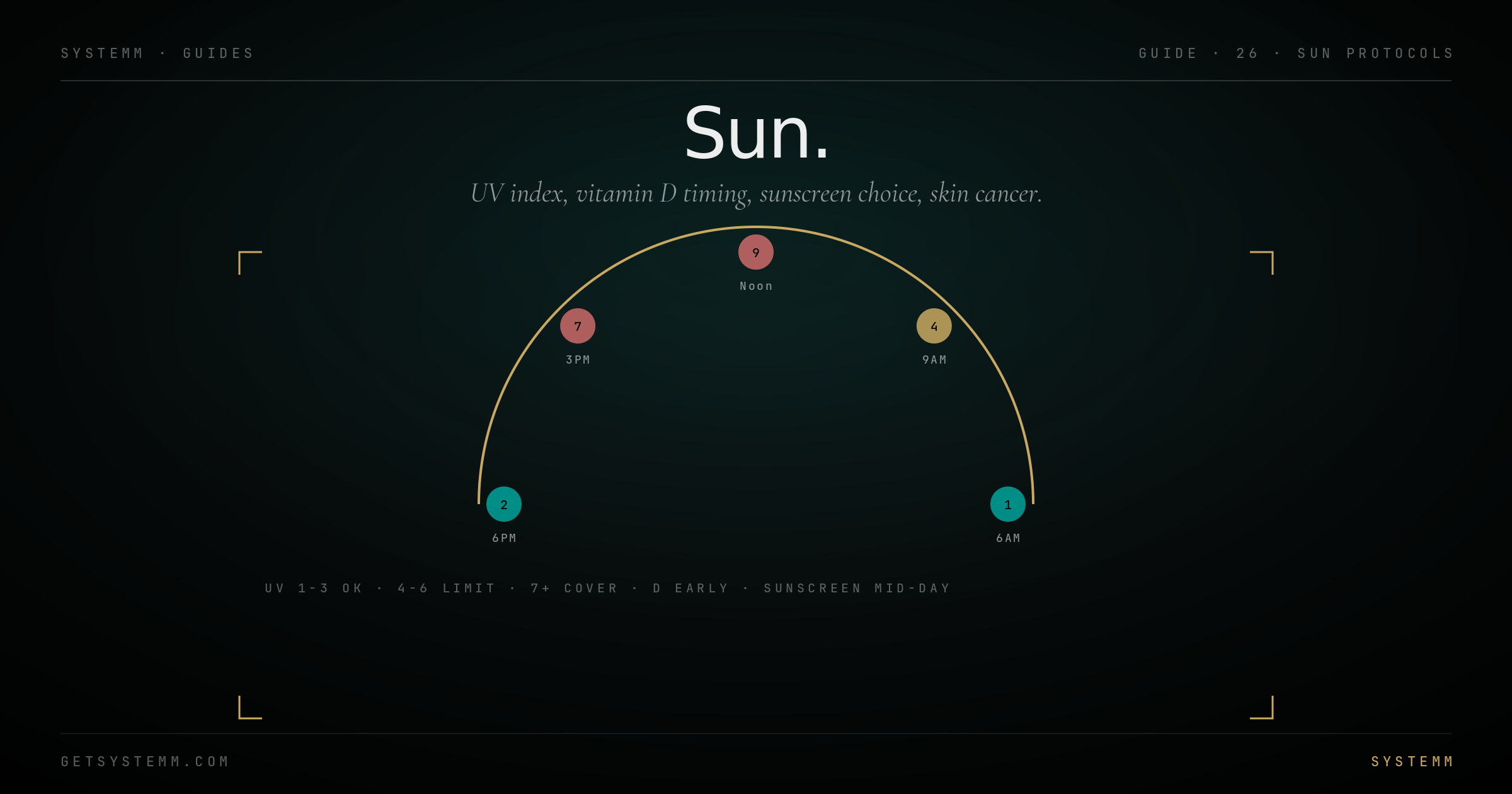
UV index is the lever. Different intensities at different times serve different functions.
UV 1-3 (early morning, late afternoon): skip sunscreen. Get 10-30 minutes of skin exposure. Burning risk is near zero. Vitamin D yield is minimal but circadian benefit is real.
UV 4-6 (mid-morning, mid-afternoon): vitamin D zone. 15-20 minutes is plenty. Sunscreen for any exposure beyond that.
UV 7+ (midday, summer, high altitude): serious burn risk. SPF 30+ on exposed skin if outdoors more than 15 minutes. Reapply every 2 hours.
UV 9+ (tropical midday): cover physically, hat, long sleeves. Sunscreen alone isn't enough.
Mineral vs chemical.
The two classes work differently. Both have trade-offs.
For daily use: mineral zinc oxide-based, SPF 30+. Brands like EltaMD UV Clear, Blue Lizard, La Roche-Posay Anthelios Mineral.
For high-UV environments: SPF 50+, water-resistant if swimming.
Reapply: every 2 hours of sun exposure, after swimming, after sweating. Most protective failures are application failures.
Once you've decided to be in the sun.
Skin cancer is mostly preventable and almost always curable when caught early. Screening cadence matters.
Self-exam monthly: shower-time inspection. ABCDE: Asymmetry, Border (irregular), Color (varied), Diameter (>6mm), Evolution (changing). Anything new or changing warrants attention.
Dermatologist full-body exam every 1-3 years if you're light-skinned, history of sunburns, or family history. Annually if you've had a melanoma or atypical nevi.
Mole-mapping photography: increasingly common, lets dermatologists compare moles to baseline. Worth doing once after age 40.
Melanotan II for tanning: produces tan via melanocyte stimulation rather than UV damage. Trade-off: not FDA-approved, side effects (nausea, libido changes, mole darkening), accelerates appearance of any precancerous lesions. Discuss with dermatologist.
Related.
For educational purposes only. Skin cancer is a medical diagnosis requiring evaluation by a dermatologist. Persistent moles, lesions, or skin changes warrant professional examination. This information does not substitute for personalized medical advice.