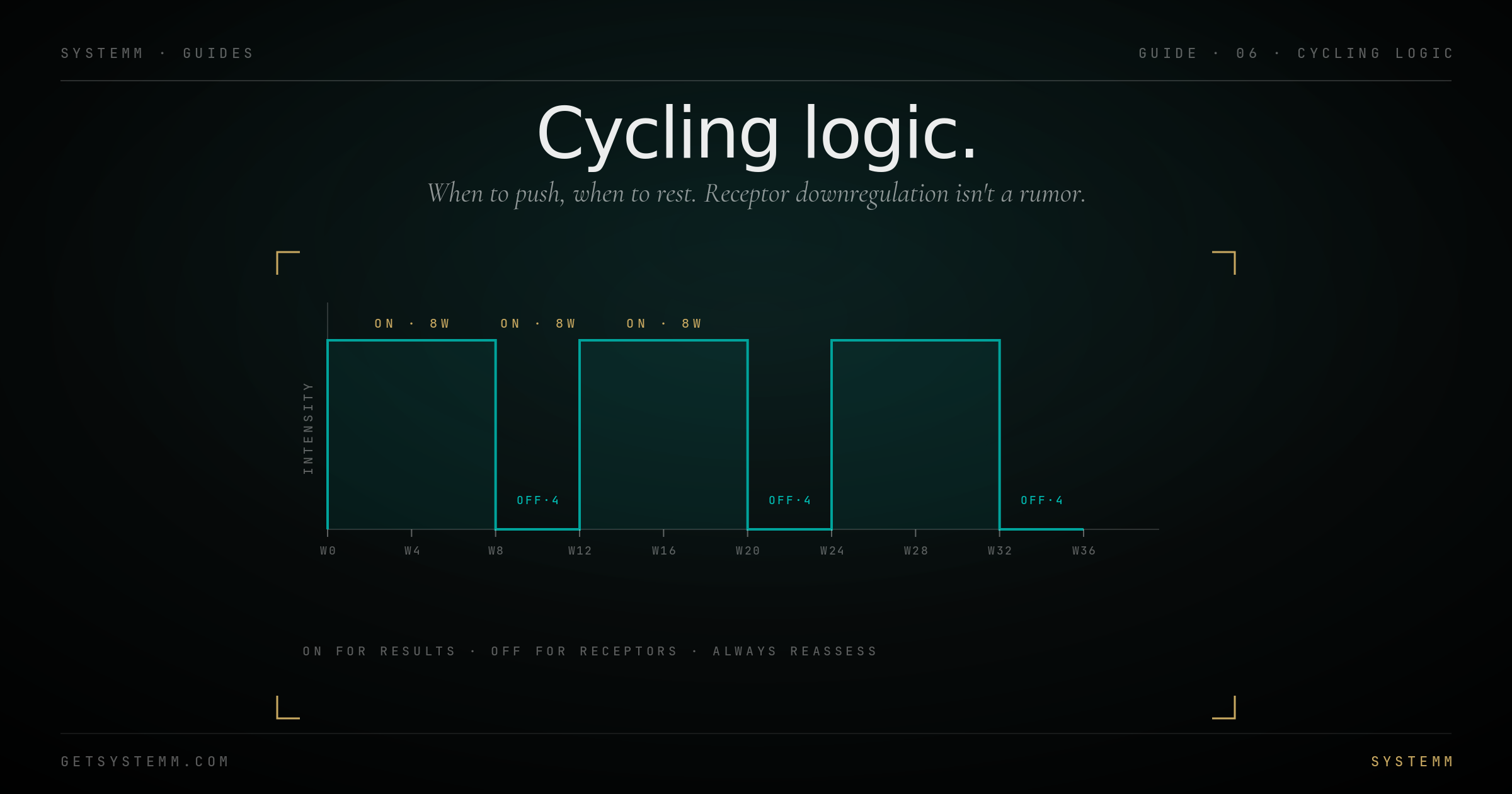
Cycling Logic.
When to push, when to rest. Receptor downregulation isn't a rumor, it's the reason chronic protocols stop working.
Receptors adapt. Always.
Every continuously-stimulated receptor downregulates. Cycling is how you keep the signal-to-noise ratio high enough that the protocol keeps working.
The body's homeostatic systems hate sustained inputs. Caffeine 8x/day for two weeks and your coffee stops working. Same molecule, same dose, less effect. The receptors are still there, they're just less responsive. This is downregulation.
Cycling restores responsiveness by removing the input long enough for the receptor system to reset. The off-period isn't wasted, it's where the protocol's future efficacy is rebuilt.
Not every compound needs cycling. Replacement hormones (TRT, thyroid) replace what the body should be making; they don't downregulate against themselves. Insulin in diabetics is replacement. The drugs that downregulate are the ones that add a signal, not replace one.
The compounds that need rest.
Stimulants, growth-hormone releasers, certain peptides, and almost anything ergogenic.
Caffeine and other stimulants: Tolerance builds in 1–3 weeks. A 2-week off-cycle every 6–8 weeks restores. Daily caffeine forever still works at a maintenance level, but acute effects shrink.
GH-releasing peptides (CJC, Sermorelin, Ipamorelin, GHRPs): 8 weeks on / 4 weeks off is the canonical pattern. Receptor sensitivity at the pituitary drops within weeks of continuous use.
SARMs and PEDs: Hard cycle compounds. 6–12 weeks on with extended off and PCT. Continuous use suppresses endogenous testosterone production and stops yielding gains.
Most performance peptides benefit from periodic breaks even if the literature doesn't formally require it. 8/4 or 12/4 is a reasonable default.
Replacement protocols are continuous.
If you're replacing something missing, you don't cycle off the replacement. Stopping creates the deficiency state.
TRT is continuous. Your body has stopped (or never made enough) endogenous testosterone, going off doesn't 'reset' anything, it puts you back in deficit.
Thyroid replacement (levothyroxine, T3) is continuous and lifelong for hypothyroidism.
GLP-1s for chronic obesity are increasingly viewed as continuous medications, similar to statins or antihypertensives. Stopping causes weight regain in most cases. Cycling them on/off produces yo-yo.
Insulin for diabetics is continuous. Never cycled.
HRT in menopause is continuous until clinical reason to stop.
- TRT, thyroid, HRT, these are replacements, not boosts.
- Insulin for diabetics, life-critical continuous medication.
- Maintenance GLP-1s for chronic obesity, stopping rebounds weight.
The shapes that actually work.
Four patterns cover 90% of needs. Pick the one that matches the compound's pharmacology.
8 on / 4 off (the default). 8-week active phase, 4-week wash-out. Used for: GH-axis peptides, most performance peptides, most stack protocols. Long enough to see results, short enough that downregulation hasn't fully set in.
12 on / 12 off (the bodybuilder). Heavier protocols, more time both on and recovering. Used for SARMs, certain PED stacks. Twelve-week off lets endogenous axes recover.
5 on / 2 off (weekly micro-cycling). Weekdays-on, weekends-off. Used for caffeine, mild stimulants, certain nootropics. Lower magnitude of break but more frequent reset.
Seasonal (twice-yearly). Long protocols (6 months) bracketed by 1–2 months off. Used for testosterone-precursor stacks, certain longevity protocols, melanotan tanning cycles.
What to do when you're off.
The off-cycle is the part most people screw up. It's not zero, it's a different protocol.
Off doesn't mean nothing. It means dropping the cycled agent while keeping the substrate intact. Sleep, training, food, stress management, all stay the same. The lifestyle base is the constant; the pharmacology is the variable.
Track during off-cycles. If your metric (strength, body comp, recovery, libido, sleep) holds during the break, you have a strong foundation. If it collapses, the cycle was masking, not improving, and you have lifestyle work to do.
Some protocols need PCT. Post-cycle therapy: HCG, clomid, enclomiphene, or similar to restart endogenous production after suppressive cycles. Required for SARMs and most PED stacks. Not needed for most peptide cycles.
Related.
For educational purposes only. Cycling protocols vary by compound, individual physiology, and goal. Some compounds require post-cycle therapy and ongoing medical monitoring. Consult a qualified physician before designing or modifying any cycle. This information does not substitute for personalized medical advice.