TRT Decision Tree.
Are you symptomatic? Have you tested? Have you tried lifestyle? Have you ruled out the alternatives? The decision sequence that prevents most regret.
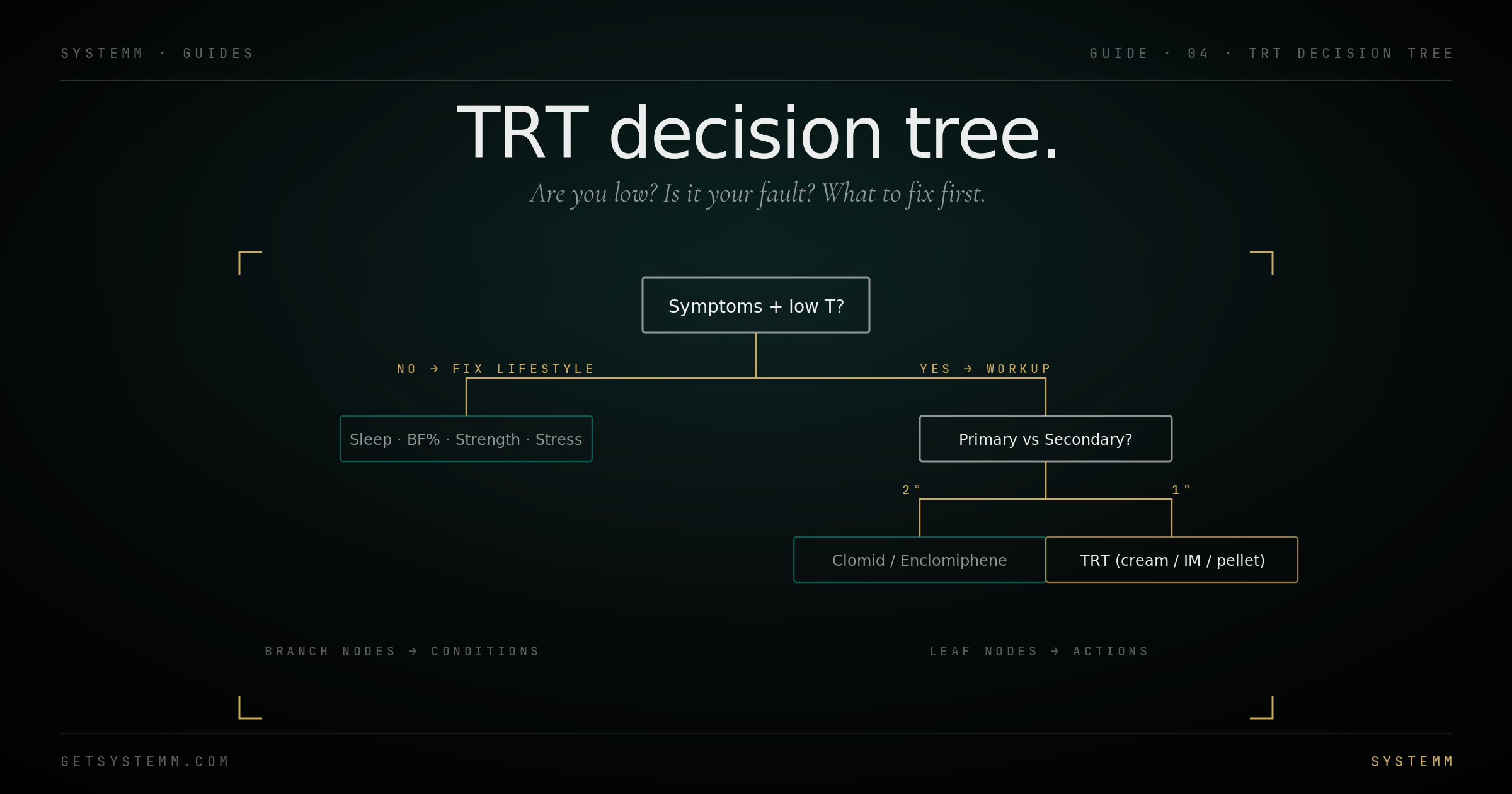
Start here, not at the lab.
TRT is a treatment for symptomatic hypogonadism. Numbers without symptoms is observation. Symptoms without numbers is something else.
The classic symptom cluster of clinical hypogonadism: persistent low libido, erectile dysfunction (especially morning erections), fatigue that doesn't improve with rest, depressed mood without obvious cause, loss of muscle mass and strength despite training, increased body fat (especially visceral), poor recovery from exercise, brain fog, reduced motivation, sleep disturbance.
The honest test: have at least 3 – 4 of these been persistent for 3+ months? Not 'I had a hard week.' Not 'I drank too much last weekend.' Persistent, multi-system, daily-life-affecting.
Symptoms != low T. Most of those symptoms overlap with: depression, sleep apnea, hypothyroidism, chronic stress, obesity, poor sleep, alcohol abuse, certain medications (opioids, SSRIs, statins in some), nutritional deficiencies. Many men feel like they have low T and actually have something else.
Two morning draws on different days.
Single readings are noisy. T can swing 30% day-to-day. Get the full hormonal picture before you decide anything.
Two separate draws, two different mornings, both between 7 – 9 AM, both fasted. A single morning testosterone reading isn't enough, natural variation can hide or fake hypogonadism. Most endocrinology guidelines require two confirming low readings before TRT.
- Total Testosterone, LC-MS/MS preferred for accuracy.
- Free Testosterone, the bioavailable fraction.
- SHBG, modifies how much free T you actually have.
- Estradiol (sensitive), LC-MS/MS. Standard immunoassay overestimates.
- LH and FSH, primary (testicular) vs secondary (pituitary) hypogonadism distinction.
- Prolactin, rule out pituitary tumor.
- DHEA-S, Cortisol AM, adrenal contribution.
- TSH, Free T4, Free T3, Reverse T3, thyroid disease mimics low T symptoms.
- CBC, CMP, lipid panel + ApoB, hsCRP, HbA1c, fasting insulin, metabolic baseline before any intervention.
- Vitamin D, ferritin, B12, magnesium, common deficiencies that worsen everything.
- PSA, baseline before starting TRT, regardless of age.
- Hematocrit, TRT can elevate it; need a baseline.
- Two separate morning draws (the single biggest mistake).
- Sensitive estradiol (regular assay gives wrong number).
- LH and FSH (determines treatment path).
- Sleep study if you snore, have erectile dysfunction, and morning headaches, undiagnosed sleep apnea suppresses T.
- Iron studies if ferritin is high (hemochromatosis can mimic everything).
Ninety days of inputs before any intervention.
The big levers can move testosterone 20 – 50% without any pharmacology. Spend 90 days on them before locking into a lifelong commitment.
- Sleep. 7 – 9 hours, dark room, cool, consistent timing. A single week of restricted sleep (5 hours) drops T 10 – 15%. Chronic poor sleep tanks it.
- Body fat. Adipose tissue aromatizes T to estradiol. Every 10 lbs of fat loss in overweight men raises T by 50 – 100 ng/dL. The single biggest lever.
- Resistance training. 3 – 4×/week. Acutely lowers T; chronically raises baseline. Compound movements (squats, deadlifts, presses) more than isolation.
- Alcohol. Even moderate chronic drinking (2 – 3 drinks daily) suppresses T. Cut to 0 – 2 drinks weekly for 90 days and re-test.
- Sugar / refined carbohydrate. Chronic hyperinsulinemia suppresses SHBG and disrupts the HPG axis. Glycemic control matters.
- Stress. Chronic cortisol elevation steals pregnenolone from T synthesis (the 'pregnenolone steal'). Address the upstream cause; meditation, breathwork, and time outdoors help.
- Vitamin D, zinc, magnesium. If deficient, replacement raises T. If sufficient, more doesn't help.
- Treat sleep apnea. If you snore, have ED, and have morning headaches, get a sleep study. Untreated apnea = chronically low T regardless of what else you do.
What numbers actually mean.
There's a single diagnostic threshold and a much larger gray zone. Be honest about which one you're in.
US clinical guidelines define hypogonadism as: total testosterone <264 – 300 ng/dL (varies by source) on two separate morning draws, plus consistent symptoms. Both required.
The gray zone, total T 300 – 500 ng/dL with significant symptoms, is where most decisions get made. The lab says 'in range.' The patient says 'I feel terrible.' This is where good medicine matters most.
Free testosterone is often more relevant than total. A man with total 500 ng/dL and SHBG 80 has low free T and will feel terrible. A man with total 500 ng/dL and SHBG 25 has normal free T and probably feels fine.
Primary hypogonadism: low T + high LH/FSH. The testicles aren't producing. Causes include genetic conditions, testicular injury, chemotherapy, aging.
Secondary hypogonadism: low T + low or normal LH/FSH. The brain isn't signaling. Causes include pituitary issues, chronic illness, opioid use, severe stress, sleep apnea, certain medications.
Treatment paths differ. Primary hypogonadism goes straight to TRT. Secondary hypogonadism in younger men can often be treated by addressing the upstream cause OR by using clomiphene / enclomiphene to stimulate the dormant axis.
The fertility-preserving alternative.
If you're younger, want to preserve fertility, and have secondary hypogonadism, try this first.
Clomiphene (Clomid) and enclomiphene work by blocking estrogen receptors at the hypothalamus and pituitary. The brain perceives 'low estrogen,' increases GnRH, which drives LH/FSH, which drives endogenous testosterone production.
The key difference from TRT: Clomid raises your own production. You don't shut down. Fertility is preserved. Testicular volume is preserved.
Enclomiphene (Androxal) is the trans-isomer of clomiphene. Clomiphene is roughly 60% enclomiphene and 40% zuclomiphene. The zuclomiphene fraction is what causes most mood and visual side effects. Pure enclomiphene = same T-raising effect, fewer side effects. Compounding pharmacy access required.
Typical dosing: Clomid 12.5 – 25 mg daily or every other day. Enclomiphene 6.25 – 12.5 mg daily. Re-test at 6 weeks.
Who it works for: men under 40 – 50, secondary hypogonadism, intact testicular function, want fertility preserved.
Who it doesn't work for: primary hypogonadism (testicles aren't responsive), men with significantly damaged HPG axis, men who've been on TRT for years.
Cream, injection, pellet, patch.
Five common delivery methods, very different pharmacokinetics, very different daily friction.
- Intramuscular injection (testosterone cypionate, enanthate, propionate, sustanon). Historical gold standard. Predictable, cheap, well-studied. 1 – 3 ml luer-lock syringe; ventrogluteal or vastus lateralis. Weekly to twice-weekly typical. Cypionate is the US standard at 200 mg/ml.
- Subcutaneous injection (same compounds, smaller insulin syringe). Same compounds, shorter needle, easier self-administration. Slightly different absorption profile but clinically equivalent for most men. Many men switch from IM to SubQ for convenience.
- Topical cream, applied daily to thin-skinned areas (inner wrist, shoulders, scrotum). No injections. Steady absorption. Transferable to others through skin contact, risk for partners and children. Often less effective in raising T than injectables.
- Pellets, small testosterone pellets implanted subcutaneously by a clinician. 3 – 6 month duration. No daily friction but inflexible, can't adjust dose mid-cycle. Mild surgical procedure for placement.
- Nasal gel, 3×/day intranasal. Approved but rarely used. Awkward dosing and lower compliance.
- Patches, older modality, skin irritation common. Largely supplanted by other forms.
Frequency, ancillaries, restart options.
- Starting dose: 100 – 150 mg/week typical for most men. Some start lower (80 mg/wk) with the plan to titrate up. Few should start above 200 mg/wk.
- Frequency: Cypionate/Enanthate twice weekly (e.g., Monday + Thursday) gives more stable levels than weekly. Daily SubQ even more stable but more friction. Propionate requires daily or EOD.
- HCG (Human Chorionic Gonadotropin), mimics LH, keeps testicles functional and fertile. 200 – 500 IU SubQ 2 – 3×/week. Increasingly hard to source legally in the US.
- Aromatase inhibitors (Anastrozole), only if E2 is elevated AND symptomatic. Most men on reasonable TRT doses don't need an AI. Over-suppressing E2 causes joint pain, dry skin, libido loss, and bone density issues. Default to no AI.
- Six-week follow-up labs, assess T, free T, E2, hematocrit. Adjust dose based on trough levels (lowest point, day of next injection).
What to track after starting.
What to watch for.
- Acne, usually transient. Often E2-driven (too high) or DHT-driven.
- Hair loss acceleration, DHT-mediated. If you're genetically predisposed, TRT often speeds it up. Finasteride / dutasteride can mitigate but introduces own risks.
- Water retention / puffy face, usually E2 elevation. Adjust dose or frequency before reaching for an AI.
- Mood swings / irritability, frequently E2 imbalance (high or low), not T itself.
- Testicular atrophy, normal on TRT without HCG. Stops endogenous T production. Reversible if you come off.
- Polycythemia, elevated hematocrit. Most common medically significant side effect. Donate blood quarterly if hematocrit climbs.
- Sleep apnea worsening, TRT can worsen existing apnea. Diagnose and treat the apnea first.
- Increased aggression, much less common than reputation suggests, but real for some. Adjust dose or frequency.
Restart, taper, or stay on?
TRT is generally a long-term commitment. Restart is possible but harder than people advertise.
Restart protocols use HCG and Clomid/enclomiphene to wake the dormant HPG axis. Typical course: HCG 1500 IU 3×/week for 4 weeks, then Clomid 25 mg daily or enclomiphene 12.5 mg daily for 4 – 6 weeks, with labs at the end.
Who restarts cleanly: men under 50, on TRT less than 5 years, who maintained HCG throughout (kept testicles functional), with otherwise healthy HPG axis.
Who doesn't: men over 60, on TRT more than 10 years, who never used HCG, with primary hypogonadism (testicles were never going to work anyway).
Expect a transition window. Symptoms during restart can be brutal, the same symptoms that drove you to TRT in the first place often return temporarily.
The honest framing: for most symptomatic men with confirmed hypogonadism, TRT is a lifelong commitment that dramatically improves quality of life. Walking away later is possible but not guaranteed. Make the start decision with that in mind.
Related.
For educational purposes only. TRT is a prescription medical treatment requiring physician supervision and ongoing laboratory monitoring. Individual response varies. The information here describes general clinical patterns and does not substitute for personalized medical advice. Consult an endocrinologist or qualified physician before pursuing any hormonal intervention.