HPG Axis.
Hypothalamus, pituitary, gonads. The three-stage control loop that decides how much testosterone you make, and the targets every TRT, fertility, or libido protocol is operating on.
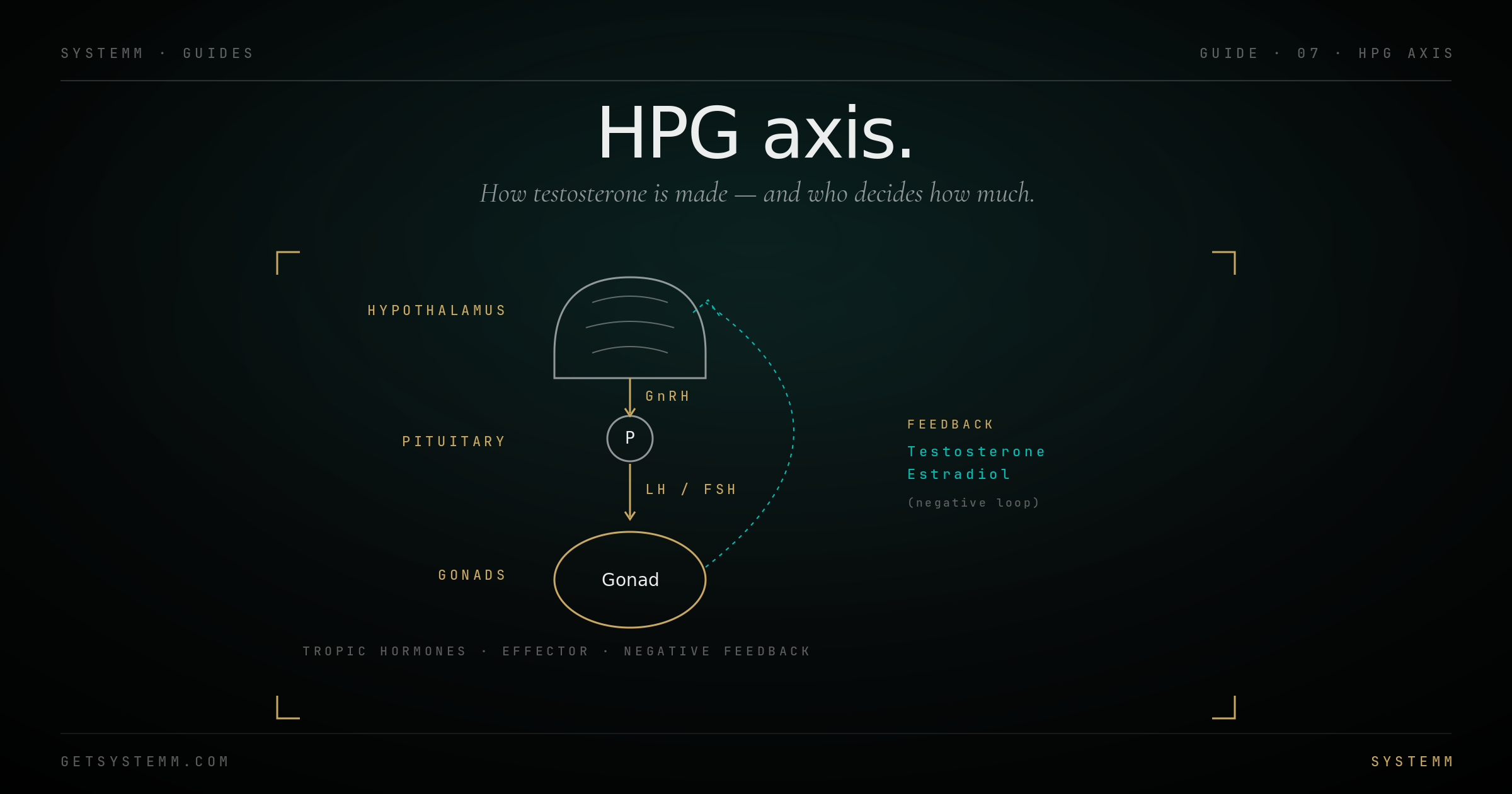
Three stages, one feedback loop.
GnRH from hypothalamus → LH/FSH from pituitary → testosterone/estradiol from gonads → feedback back to top.
The hypothalamus is the conductor. It releases pulses of GnRH (gonadotropin-releasing hormone) every 60–120 minutes. The pulse pattern, not the total amount, is what triggers the next stage. Continuous GnRH actually suppresses the axis, the reason GnRH agonists like leuprolide are used as chemical castration in prostate cancer.
The pituitary is the amplifier. GnRH pulses bind to the anterior pituitary, which releases LH (luteinizing hormone) and FSH (follicle-stimulating hormone) into the bloodstream. LH drives steroidogenesis; FSH drives gametogenesis.
The gonads are the factory. In men, LH stimulates Leydig cells in the testes to produce testosterone; FSH stimulates Sertoli cells to support sperm production. In women, FSH drives follicle development and LH triggers ovulation and corpus luteum function.
The feedback loop closes the system. Testosterone and estradiol from the gonads suppress GnRH at the hypothalamus and LH/FSH at the pituitary, high T = less LH = less T production. This is why exogenous testosterone shuts down endogenous production.
What each stage actually does.
Knowing which stage is broken tells you which intervention will work.
Primary hypogonadism (gonadal failure): low T, high LH/FSH. Brain is shouting but factory is broken. Causes: testicular trauma, mumps orchitis, chemotherapy, Klinefelter's. TRT is the only effective treatment.
Secondary hypogonadism (hypothalamic-pituitary): low T, low or inappropriately normal LH/FSH. Factory is fine but no one's calling. Causes: pituitary tumor, hyperprolactinemia, stress, obesity, chronic illness, opioid use. Often reversible by treating the underlying cause; clomid/enclomiphene also work by restoring the signal.
What your hormone panel tells you.
Total T tells you the level. LH/FSH tells you why.
Total testosterone is the headline number. Reference ranges are wide (commonly 264–916 ng/dL for adult males) and clinically misleading, symptoms often appear at the bottom of 'normal.' Optimal generally sits 600–900 ng/dL for adult men.
Free testosterone is the bioavailable fraction. Total T can be normal while free T is low if SHBG is elevated. Always check both.
LH and FSH distinguish primary from secondary. Low T with high LH = gonadal failure. Low T with low LH = central failure.
Estradiol (sensitive assay) is required, especially on TRT. E2 too low: low libido, joint pain, mood drop. E2 too high: emotional lability, water retention, gynecomastia risk. Target 20–40 pg/mL.
SHBG binds testosterone and reduces free fraction. Affected by thyroid, insulin resistance, alcohol, body fat.
What moves what.
Different problems need different tools. Pick the level you're trying to fix.
Lifestyle interventions work at the hypothalamic level. Sleep deprivation, chronic stress, obesity, and overtraining suppress GnRH. Fixing these often resolves mild secondary hypogonadism without medication.
Clomiphene / Enclomiphene are selective estrogen receptor modulators that block estrogen's feedback at the hypothalamus, the brain perceives low estrogen and ramps up GnRH, increasing LH and endogenous testosterone. Best for secondary hypogonadism with intact testicular function.
HCG (human chorionic gonadotropin) mimics LH and stimulates the testes directly. Used to maintain testicular size/fertility on TRT, or to restart endogenous production post-cycle.
Exogenous testosterone replaces the end product but shuts down the entire upstream axis. Useful when the goal is restoration; problematic if fertility is a priority.
- Estradiol management on TRT, over- and under-suppression both cause symptoms.
- Hematocrit and PSA monitoring every 6 months on continuous TRT.
- Fertility implications, discuss HCG co-administration if you want options.
Related.
For educational purposes only. Hormonal disorders require physician diagnosis and supervision. Lab interpretation is context-dependent. This information does not substitute for medical evaluation by a qualified endocrinologist or hormone specialist.