Female Hormone Primer.
The menstrual cycle as a biomarker, perimenopause, HRT options. GLP-1 considerations for women.
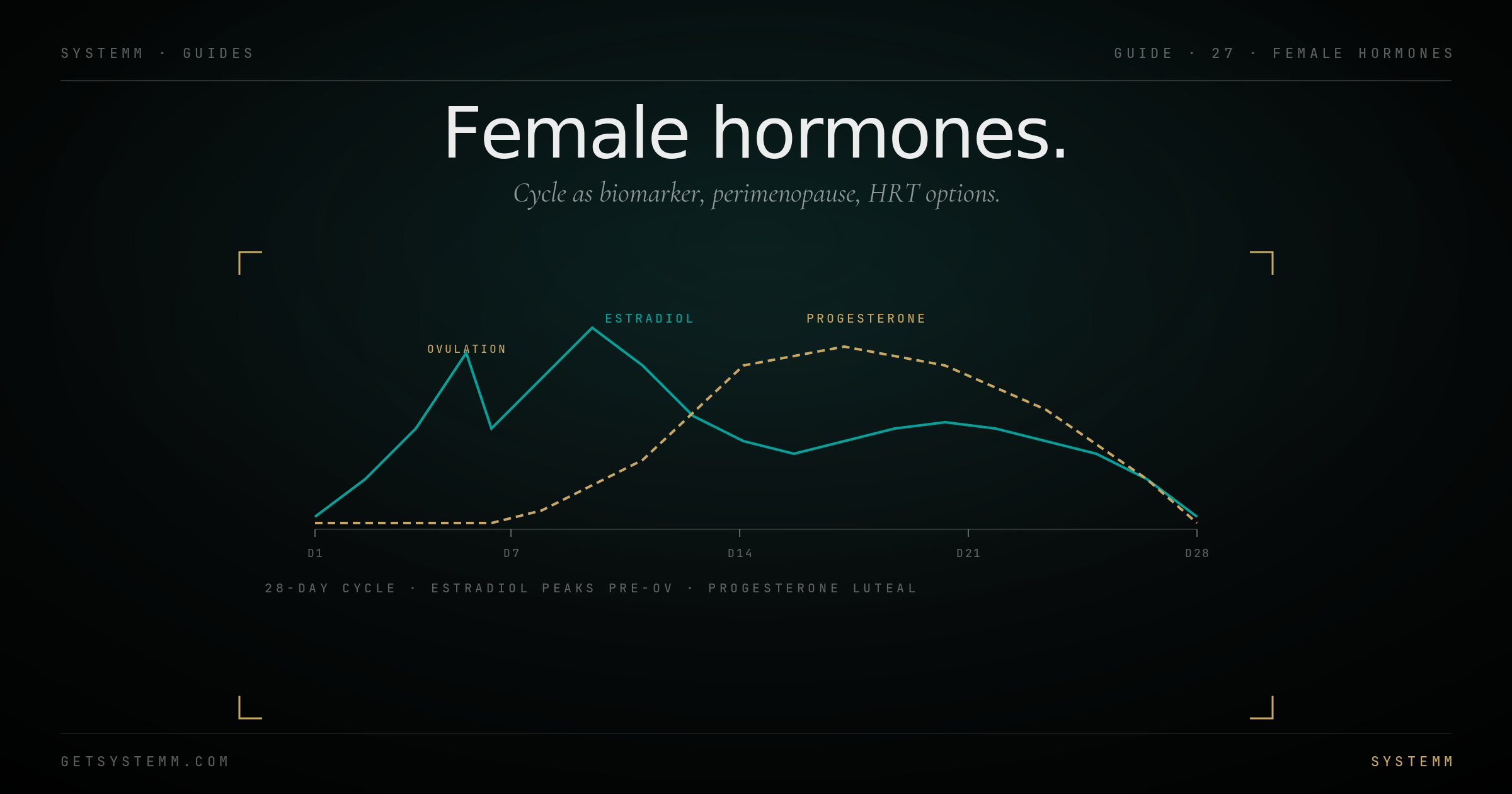
28 days, four phases.
Cycle regularity is one of the strongest biomarkers a woman has. Pattern changes mean something.
Days 1-5 (menses): estrogen and progesterone at lowest. Energy often low. Iron loss happens here, keep ferritin in check.
Days 6-13 (follicular): estrogen rises. Energy, mood, strength all favor this window. Best week for hard training.
Day 14 (ovulation): estrogen peaks, LH surges. Brief libido spike. Basal body temp jumps ~0.5°F (visible on Oura ring temperature data).
Days 15-28 (luteal): progesterone dominant. Body temperature elevated. Some women experience PMS or PMDD in late luteal phase.
What irregularity means: cycles longer than 35 days or shorter than 21, missed periods, very heavy bleeding, severe pain, all warrant workup. Common causes: PCOS, thyroid, perimenopause, hypothalamic amenorrhea (from low body fat, overtraining, or undereating).
The 5-10 year transition.
Begins late 30s to mid 40s. Often dismissed. Worth understanding because protocols start here.
Hormonal pattern: progesterone declines first (luteal-phase insufficiency), then estrogen becomes variable (often higher than normal, then low). The variability itself causes symptoms.
Symptoms: cycle length changes, sleep disturbances (often the first symptom, especially mid-cycle), hot flashes, mood changes, weight gain (often abdominal), brain fog, libido changes.
Workup: FSH (elevated suggests perimenopausal/menopausal), estradiol, progesterone (best mid-luteal phase), testosterone, DHEA-S, thyroid panel, vitamin D, B12, ferritin. AMH if fertility is still a question.
The trap: 'normal' labs are common in early perimenopause because labs sample one day in a highly variable system. Symptoms are valid evidence even when one-day labs aren't dramatic.
What's available, what works.
Modern HRT is bioidentical, transdermal where possible, dosed to symptoms not arbitrary numbers.
Estradiol, transdermal patch, gel, or pellet. Transdermal lower clot risk than oral. Dose to symptoms: hot flashes resolved, sleep improved, vaginal symptoms gone.
Progesterone, oral micronized progesterone (Prometrium) at night, 100-200mg. Sedating (sleep benefit). Required if you have a uterus and are taking estrogen (uterine cancer protection).
Testosterone, increasingly recognized in women. Cream or pellet at female doses (1/10 male dose). Improves libido, energy, mental clarity, lean mass.
DHEA, adrenal precursor. Some women find it helpful, others don't. Modest evidence.
The Women's Health Initiative (2002) scared a generation off HRT. The original interpretation was wrong; modern transdermal bioidentical HRT in women under 60 has much better risk-benefit. The cancer / cardiovascular fears applied largely to oral conjugated equine estrogens started 10+ years after menopause.
Two considerations.
Muscle preservation is more critical for women. Lower starting lean mass; loss is harder to rebuild. Resistance training 3x/week is non-negotiable on GLP-1s.
Estrogen-GLP-1 interactions exist. Some women on HRT report mood and appetite shifts when starting GLP-1; protocols are still evolving.
Fertility: GLP-1s are contraindicated in pregnancy. Discontinue 2+ months before trying to conceive. Improves PCOS-related infertility in some users via metabolic effects on ovulation.
Bone density: rapid weight loss in postmenopausal women accelerates bone loss. DEXA bookends and resistance training are protective.
Related.
For educational purposes only. Women's hormone health requires individualized medical evaluation. HRT decisions involve personal risk-benefit assessment with a qualified clinician (gynecologist, endocrinologist, or hormone specialist). This information does not substitute for personalized medical advice.