Hair Loss Decision Tree.
Diagnose the pattern, then pick the right lever. Five-year timelines. Document the baseline before you change anything.
AGA is most common, but not the only cause.
Pattern, timeline, and family history distinguish androgenetic alopecia from other causes.
Androgenetic alopecia (AGA, male/female pattern) is the dominant cause, gradual, follows Norwood (men) or Ludwig (women) patterns, often family history. DHT-mediated miniaturization of scalp follicles. Treatable but progressive without intervention.
Telogen effluvium: diffuse shedding 3 months after a major stressor (illness, surgery, childbirth, severe weight loss, emotional shock, certain medications). Usually self-resolves within 6–12 months once stressor passes.
Alopecia areata: autoimmune patchy hair loss. Round bald patches that appear quickly. Distinct from AGA. Treated by dermatologist, typically with steroids or JAK inhibitors.
Nutritional / medical: iron deficiency (ferritin <40 ng/mL), thyroid dysfunction, severe vitamin D deficiency, recent crash diet. Treat the underlying cause; hair follows once corrected.
Traction alopecia: from repeated tension (tight ponytails, weaves, certain styling). Reversible if caught early.
What actually works for pattern hair loss.
Four tiers of intervention, ordered by evidence strength. Most users land on a combination.
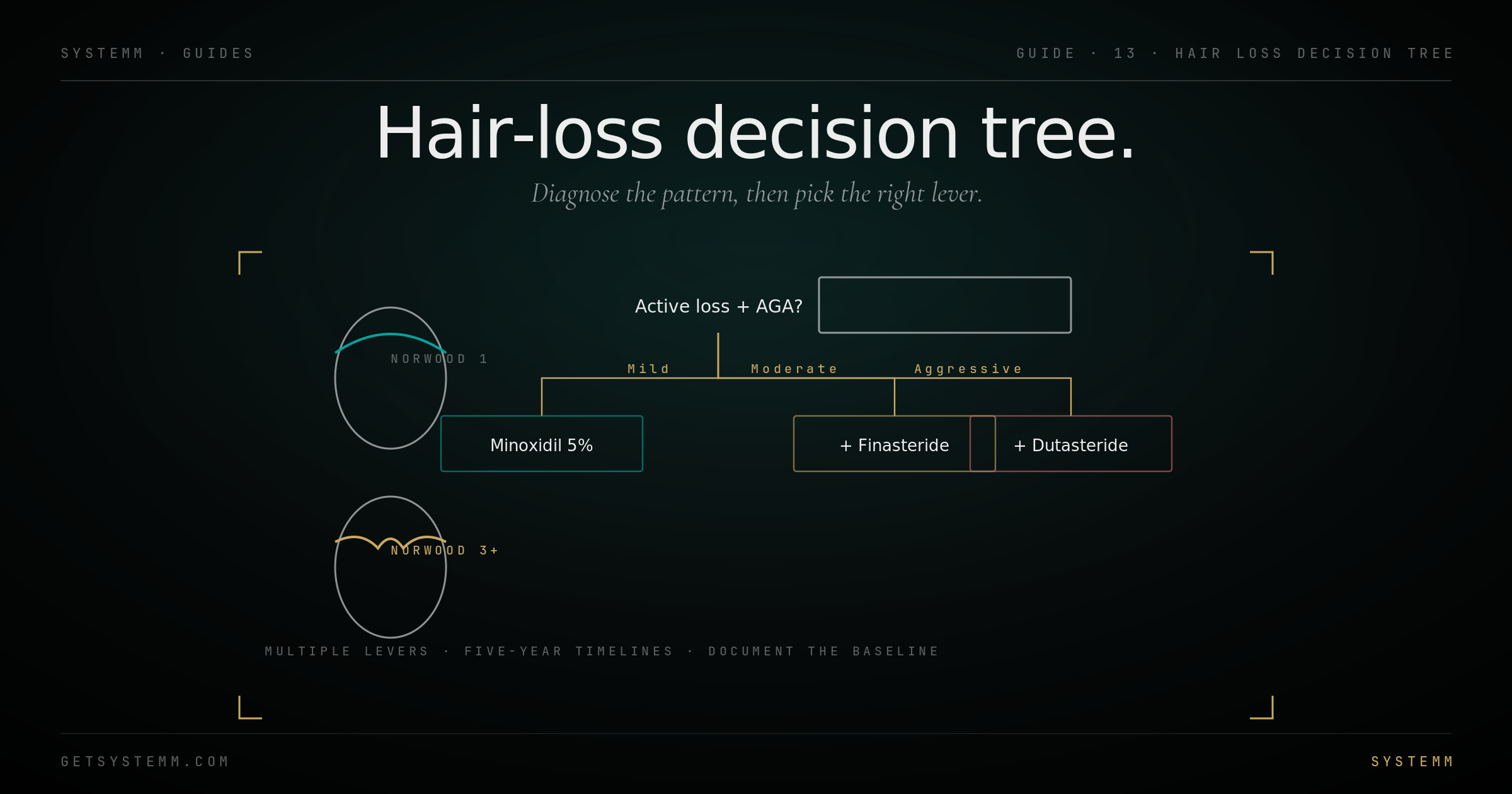
Standard combination protocol for moderate AGA: Topical minoxidil 5% twice daily + oral finasteride 1mg daily + microneedling weekly. 12 months minimum to evaluate response. ~80% of users see measurable improvement at this stack.
For aggressive loss: Add dutasteride 0.5mg (replaces finasteride) and/or oral minoxidil. Discuss with a dermatologist or hair-focused physician.
Hair takes longer than you think.
The follicle cycle is months. Improvement compounds slowly. Quitting at 3 months is the most common protocol failure.
Month 0–2: Initial 'shed', counterintuitively, minoxidil causes more hairs to enter the shed phase faster, before regrowth. Many users panic and quit. Wrong move.
Month 3–6: First visible regrowth at the hairline and crown. Hairs at this stage are thin and short ('vellus'). Improvement is real but easy to miss.
Month 6–12: Density improvement. Photos at 12 months vs baseline tell the truth.
Month 12–24: Maximum effect plateau. What you have at 24 months is roughly what you'll keep, provided you continue the protocol indefinitely. Stopping returns to baseline within 12 months.
Year 3+: Maintenance. Continue the protocol that got you there. Periodic photos confirm the result is holding.
What to watch for, what's overblown.
Finasteride sexual side effects are real but rare. Minoxidil shedding is expected. Most concerns are manageable.
Finasteride sexual side effects (reduced libido, ED, ejaculation issues) affect 1–4% of users in placebo-controlled trials, with much of the effect arguably nocebo-driven. Most are reversible on stopping. Post-finasteride syndrome (PFS), persistent side effects after discontinuation, exists but is rare and poorly characterized.
Topical finasteride reduces but does not eliminate the systemic absorption that drives sexual side effects. Some absorption still occurs.
Minoxidil scalp irritation: switch to foam (less alcohol) or to oral minoxidil. Initial shedding is expected and resolves.
Oral minoxidil at 2.5–5 mg: peripheral edema in some users, mild hypertrichosis (extra body/facial hair) in women especially. Generally well-tolerated.
Dutasteride: same side effect profile as finasteride but slightly higher rates; longer half-life means side effects persist longer on discontinuation.
- Family history of prostate cancer (5α-RIs reduce PSA, complicate screening).
- Current heart disease (oral minoxidil cardiovascular profile).
- Pregnancy or trying to conceive (women: 5α-RIs are teratogenic).
- Hair loss in patches (suggests alopecia areata, not AGA).
Related.
For educational purposes only. Hair loss treatments, particularly finasteride and dutasteride, are prescription medications with potential side effects requiring physician oversight. Photo documentation is essential to honest evaluation. This information does not substitute for evaluation by a dermatologist or hair-focused physician.