HPT Axis.
Hypothalamus, pituitary, thyroid. The metabolic thermostat. Why energy comes and goes, and why thyroid replacement is a different kind of decision than TRT.
The metabolic dimmer switch.
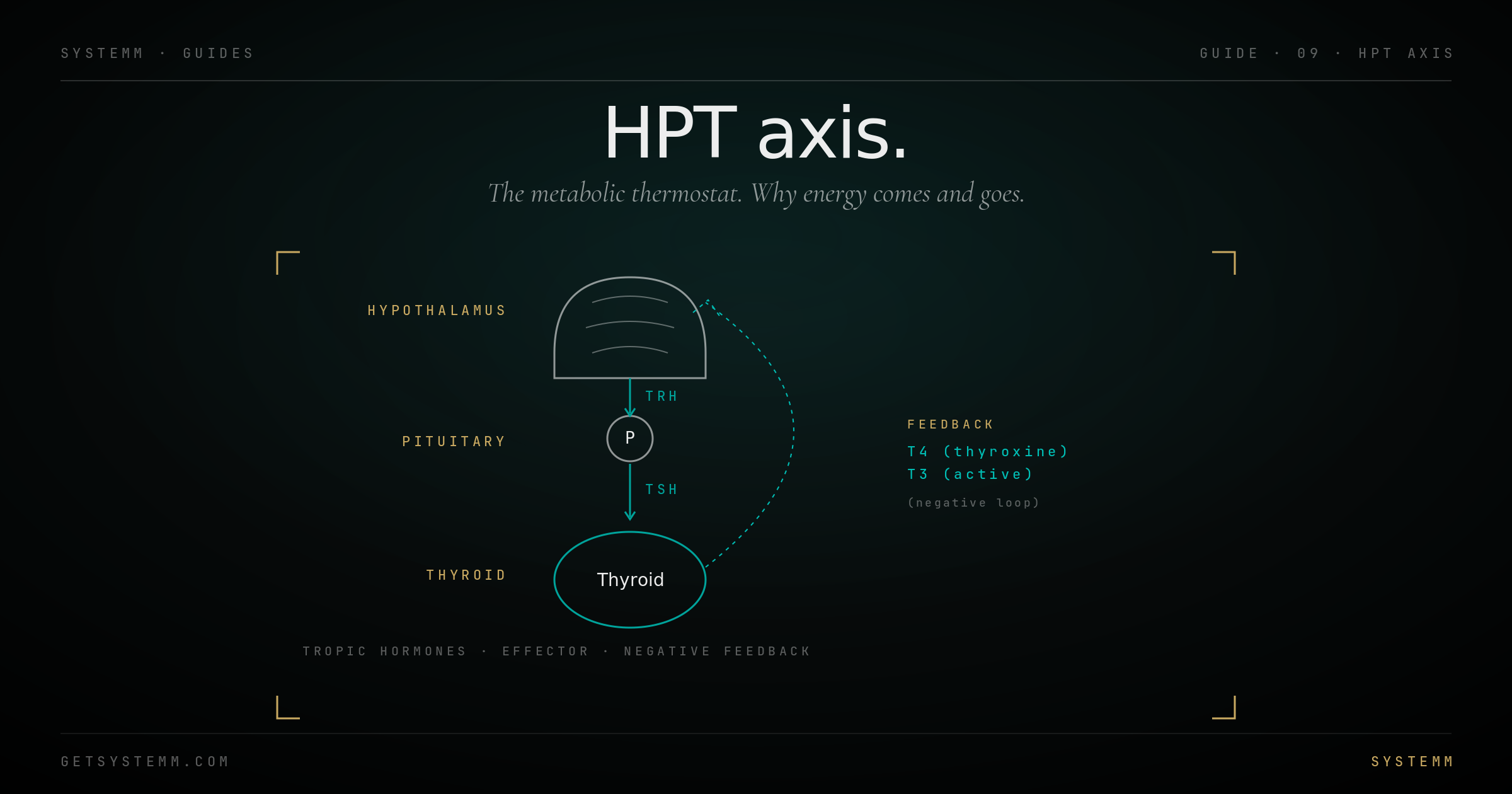
TRH → TSH → T4 → T3. T3 is the molecule that actually does the work.
The thyroid axis sets your metabolic rate. The hypothalamus releases TRH (thyrotropin-releasing hormone). The pituitary responds with TSH (thyroid-stimulating hormone). The thyroid gland produces T4 (thyroxine, mostly inactive) and a small amount of T3 (triiodothyronine, the active hormone).
T4 is a pro-hormone. Most active thyroid hormone (T3) is generated by peripheral deiodinase enzymes converting T4 to T3 in target tissues. The liver, kidney, and to some extent the brain do most of this conversion.
T3 binds thyroid hormone receptors in nearly every cell, driving gene expression that controls mitochondrial activity, protein synthesis, lipid metabolism, body temperature, heart rate, and brain function. It's the closest thing the body has to a master metabolic dial.
Negative feedback from T4 and T3 (and other inputs like inflammation, cortisol, leptin) shuts down TRH and TSH when levels are sufficient.
Too little, too much, or wrong conversion.
Three failure modes, three sets of symptoms, three workups.
Hypothyroidism (too little thyroid hormone). Causes: Hashimoto's autoimmune thyroiditis (most common), iodine deficiency, post-surgical, post-radiation, certain medications. Symptoms: fatigue, weight gain, cold intolerance, brain fog, dry skin, hair thinning, constipation, depression. Lab pattern: high TSH, low free T4 and T3.
Hyperthyroidism (too much). Causes: Graves' disease (autoimmune stimulating antibodies), toxic nodule, thyroiditis. Symptoms: weight loss, heat intolerance, palpitations, anxiety, tremor, insomnia, frequent stools. Lab pattern: low TSH, high free T4 and/or T3.
Conversion deficits. 'Normal' TSH and T4 but persistently low free T3, often paired with low rT3 or low reverse-T3-to-T3 ratio. Driven by chronic inflammation, severe caloric restriction, illness, or genetic deiodinase variants. Standard medicine often misses this pattern; functional medicine emphasizes it.
What a full thyroid panel actually shows.
TSH, free T4, free T3, reverse T3, plus antibodies for autoimmune workup.
What's available, what works.
Levothyroxine is standard. T3-containing options exist for non-responders. Lifestyle inputs matter more than people think.
Levothyroxine (T4 monotherapy) is the standard. Easy to dose, long half-life, predictable. Works for ~80% of hypothyroid patients. The other 20% don't convert T4 to T3 well and continue to feel symptomatic with 'normal' labs.
Liothyronine (T3) added or as monotherapy: for non-responders. T3 has a short half-life (~12 hours) so usually dosed twice daily. Risk of cardiac arrhythmia if overdosed; requires monitoring.
Desiccated thyroid extract (NDT, Armour, Nature-Throid): porcine thyroid containing T4, T3, T2, T1, calcitonin. Many patients prefer this; absorption and dosing slightly less predictable than levothyroxine.
Lifestyle inputs that matter: adequate iodine (seaweed, dairy, iodized salt), selenium (Brazil nuts, fish, required for deiodinase enzymes), avoiding chronic caloric restriction (drops T3 within days), addressing chronic inflammation (which suppresses T3 conversion), treating sleep apnea (independent thyroid suppressor).
- Take thyroid medication on empty stomach, 30–60 min before food. Coffee, calcium, iron, and fiber all impair absorption.
- Lab draws should be consistent: same time of day, before or after dose consistently, not a moving target.
- Recheck labs 6 weeks after any dose change; longer is required for steady state.
Related.
For educational purposes only. Thyroid disease is a medical diagnosis requiring physician evaluation and treatment. Self-prescribing thyroid hormones is dangerous. This information does not substitute for evaluation by a qualified endocrinologist or thyroid specialist.